
Predicting Together to Prevent: Fall Prevention in the Achterhoek
October 2025This article was originally published in Dutch on Datawerkplaats.net. For your convenience, we have translated it here.
In conversation with Paul van der Meer, Health Promotion Advisor at GGD Noord- en Oost-Gelderland, and Yvanka Klein Holte, District Nurse and Nursing Researcher at Sensire.
Most falls among the elderly are preventable, yet often have significant consequences for health and healthcare costs. A fall can mark the beginning of a long recovery period, loss of independence, and higher care costs. In the Achterhoek region, municipalities, healthcare and welfare organizations, and the public health service (GGD) are pooling their knowledge and data to identify fall risks earlier and better support the elderly with preventive interventions.
During Fall Prevention Week, we spoke with Paul van der Meer and Yvanka Klein Holte. Together they provide insight into the GERDA (Integrated Regional Data Infrastructure Achterhoek) Fall Prevention Chain Approach.
“We record a lot of data, but we don’t use it optimally yet. The information is often fragmented—I record something, the GP records something else, the physiotherapist records something different again. Especially around fall prevention, we can gain a lot by better connecting this data.”
— Yvanka Klein Holte, District Nurse and Nursing Researcher at Sensire
The Impact of a Fall
Klein Holte explains that falling can have an enormous impact on the lives of elderly people living at home: “Not only on the individual, but also on society and their network. When someone falls, even without breaking anything, the network and caregivers must spring into action. Initially acute when someone can’t get up anymore, but also in the longer term. Let alone when someone does break something and ends up in the entire healthcare system.”
At Sensire, they see an 11% increase in care hours after someone falls. Klein Holte: “And in the 10 weeks before someone falls, you already see an increase in hours. It has also been observed that when someone falls once, 50% fall a second time.”
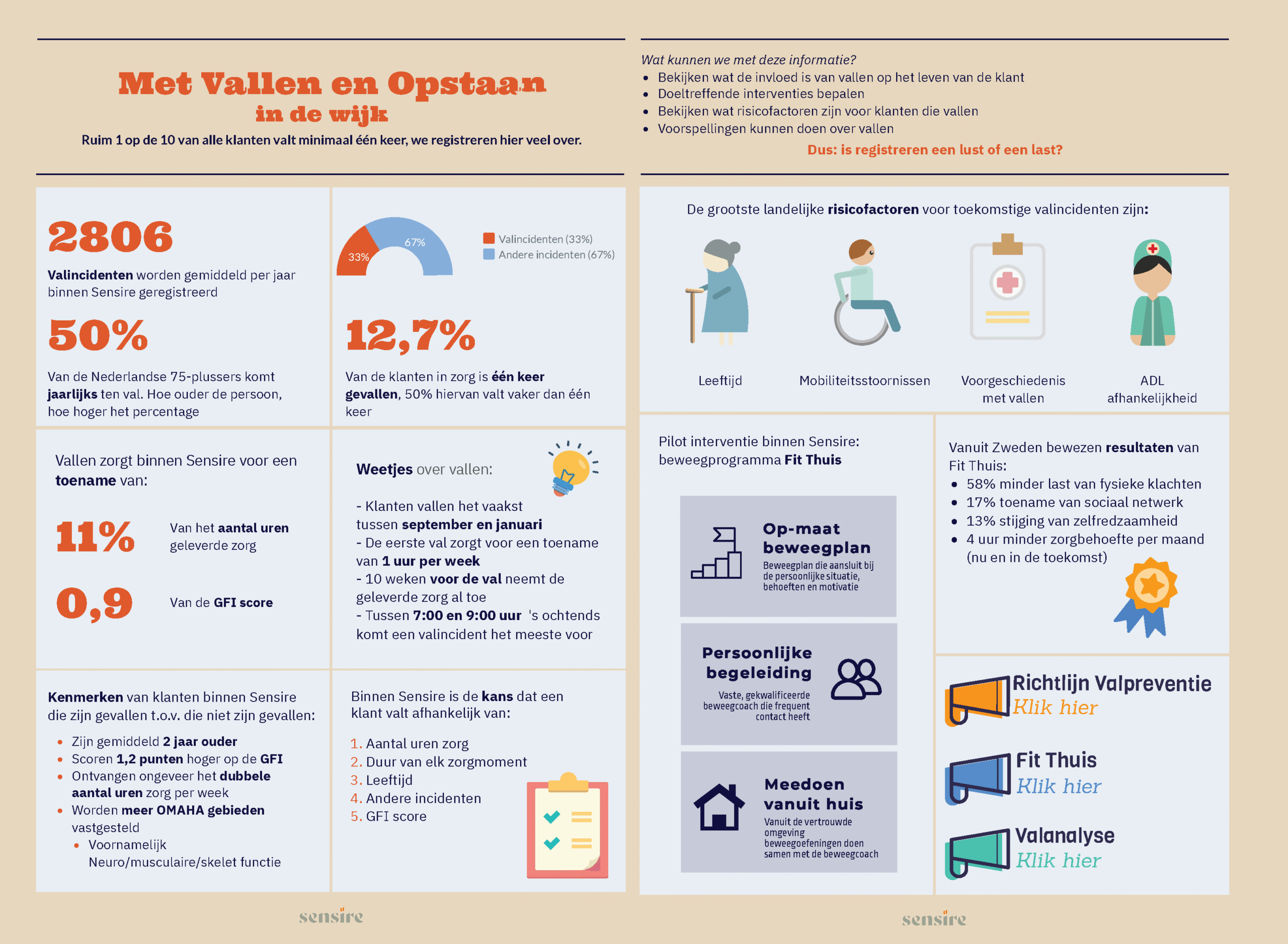
Figure 1: Fall data from Sensire
Regional Collaboration for Fall Prevention
In 2023, regional collaboration around fall prevention started in the Achterhoek. Paul van der Meer joined as regional project leader, commissioned by the eight Achterhoek municipalities and health insurer Menzis. “I see myself primarily as someone who facilitates that process with all those organizations. Think of representatives from general practitioners, municipalities, Menzis, Proscoop, PMA (Paramedi Achterhoek), Achterhoek in Beweging, NOVA, and the East Achterhoek Pharmacists Association. All these parties record valuable data, but often separately. The idea is to bring that data together to map which groups have an elevated fall risk. Together we work on regional agreements and ensure good local implementation. This creates a more complete picture of elderly people with elevated fall risk, making it easier to intervene timely and targeted.”
Yvanka Klein Holte also plays a key role in this project. From her role as district nurse, nursing researcher, and data steward, she bridges the gap between daily care practice and data analysis: “Within GERDA, I mainly fulfill a content-related role, analyzing which issues are at play and whether they align with practice. What is helpful in this, which question should we answer together, and who should we involve.”
Klein Holte sees great opportunities in better utilizing healthcare data. “We record a lot, but we don’t use that data optimally yet. The information is often fragmented—I record something, the GP records something else, the physiotherapist records something different again. Especially around fall prevention, we can gain a lot by better connecting this data.”
The Four Steps of the Chain Approach
The collaboration in the Achterhoek aligns with the national fall prevention chain approach, developed by VeiligheidNL and established in the Integral Care Agreement (IZA) and the Healthy and Active Living Agreement (GALA). Van der Meer explains that the approach consists of four steps: “First, there’s detecting and signaling risks. Then follows a screening phase to see how high the fall risk is. Next comes the intervention.” Klein Holte elaborates: “If the problem is with vision, you go to the optician. If it’s about proper footwear, you give advice about that or refer to a podiatrist. If it’s about medication, then to the GP. And if it’s about strength and mobility, physiotherapy or for example a gym group is appropriate. If the cause remains unclear, some hospitals have a fall clinic for further assessment.”
A Federated Learning Model
Within the GERDA data workshop, they work with a federated learning model: a privacy-friendly and predictive form of machine learning where data stays at its own location. The model is brought to the data, so only anonymized results are shared instead of sensitive information. This way, organizations can make predictions together without sharing their data.
Klein Holte: “We also use descriptive statistics to identify target groups and describe characteristics, and look at whether we can steer more specifically based on that.”
Van der Meer: “Currently, we often send invitations for fall risk tests to everyone. That works, but it also feels a bit like shooting with buckshot. With data from GERDA, we could invite much more targeted and reach the right people.”
This creates an approach that not only reduces registration burden but also deploys capacity in the chain more smartly. Klein Holte emphasizes: “Falling is a complex societal issue. Only by working together across disciplinary boundaries can we not only manage risks but also consciously accept them, so that the right care ends up in the right place.”
“I hope that in five years we’ll still be learning, based on objective data. That all organizations working with people 65 and older share their data and that registration systems are better connected. And that there is trust in the collaboration between all involved actors within the chain.”
— Paul van der Meer, Health Promotion Advisor at GGD Noord- en Oost-Gelderland
Learning from Each Other
Although the approach is being developed in the Achterhoek, other regions could also learn from it. Van der Meer: “I think the insights we gain here can easily be copied to other regions. At the GGD, we already exchange a lot anyway. Every region has its own context, but the analysis setup is well reusable.”
Klein Holte: “Every region works in its own way, but with the background information and context of how and which data we use, this approach is well applicable. Other regions can then adapt it to their own situation.”
Looking Ahead
The Fall Prevention Chain Approach is a matter of perseverance. It’s about behavioral change among residents, good preparation and support of practitioners, and structural collaboration between healthcare and social domains, supported by digital referral and communication systems. Van der Meer: “I hope that in five years we’ll still be learning, based on objective data. That all organizations working with people 65 and older share their data and that registration systems are better connected. And that there is trust in the collaboration between all involved actors within the chain.”
Klein Holte adds: “I hope we have insight into each other’s data and can utilize it. So that GPs, physiotherapists, hospitals, and district nursing don’t have to register twice. With combined data, AI can predict elevated fall risks, so professionals can intervene earlier.”
Source: Datawerkplaats.net